Latest News
WHAT IS CONFLICT?
There are several definitions of conflict. The one I like describes it as an "ongoing process of variable intensity involving multiple interactions over time in which people not only have differing and sometimes incompatible views of facts, goals, methods, or values but sense interference from one other in the achievement of valued outcomes". Conflicts can be adaptive or maladaptive, functional/constructive or dysfunctional. Indeed human and societal progress over the ages, for example, has been driven by conflict. But the liquidation of entire peoples and cultures has also been driven by conflict. The outcome of a given conflict, therefore, depends on how it is managed by contending forces. Lack of social reciprocity and/or tolerance for differences of opinion increases the risk of violence and war.
Over the last 15 years, African disasters due to conflicts have accelerated in comparison with those due to natural causes and epidemics. All over the world, violence is second only to respiratory diseases as a cause of lost life expectancy.
WHAT ARE THE ENABLING FACTORS BEHIND CONFLICTS IN AFRICA?
In a recent landmark report to the Security Council, the Secretary General of the United Nations, Kofi Annan, reflected on a number of causes of conflict in Africa. They include historical legacies such as the Berlin conference of 1885, the scramble to divide Africa among European powers (without regard for ethnic realities), and the subsequent establishment of colonial commercial and political structures designed primarily to extract resources. Against this background, Africa became one of several locations in the world where super-power rivalries played out during the cold war. In the setting of a central strategic stalemate in Europe, cold war antagonists tried to outflank one another in Africa, Asia and South America, using local players as pawns. As if this was not enough, the end of the cold war was associated with a rebound phenomenon, in which long suppressed rivalries resurfaced at a time of declining international focus and attention, but nevertheless fueled by excess weapons from cold war stocks. Other external factors include economic motives on the part of arms merchants, foreign state and non-state actors (like multinational corporations). But all of Africa's problems cannot be blamed on external factors. Internal factors that promote conflict include the nature of power on the continent, a winner-takes-all mentality, zero-sum political games, centralization and personalization, lack of accountability, lack of transparency, lack of rule of law, lack of peaceful transitional mechanisms and absence of human rights, all of which are set against poverty, lack of education and a primordial background of deep rooted ethnic and religious mindsets. And then we must not forget cofactors like conflict creating environmental problems such as water and land shortage and environmental degradation.
In a draft report on the subject a few years ago, the OAU identified certain contributing factors to 26 conflicts affecting over 60% of the population between 1963 and 1998. These included ethnicity in Rwanda and Burundi, power-sharing in the DRC-1998, Sudan-1983, Sao Tome/Principe 1994 and Comoros 1995, inter-clan and other factional rivalries in Somalia, Liberia and Guinea Bissau, mercenaries in the DRC 1964, Guinea 1970 and Benin 1977, human rights violations under Idi Amin in Uganda from 1970-79 and cold war geopolitics in Chad 1977-80 and Mozambique 1975-92. In the post cold war era, however, I am attracted to the classification of African conflicts proposed by Tom Lodge:
ethnic competition for control of the state; for example, Nigeria
regional or secessionist rebellions; for example, Sudan, Senegal
continuation of liberation conflicts; for example, Angola, Western Sahara
fundamentalist religious opposition to secular authority; for example, Algeria
warfare arising from state degeneration or state collapse; for example, Somalia, Sierra Leone, Congo-DRC
border disputes; for example, Ethiopia-Eritrea
protracted conflict within politicized militaries, for example, Congo-DRC, Sierra-Leone Conflict types can be major or minor, superficial or deep-rooted, short term or long term, and they can overlap. A country like Nigeria, for example, has a variety of low grade conflicts that result in chronic blood letting without the country actually being in an open declared state of war. It keeps the country off balance.
Once conflict become violent, it takes on a different level of dysfunctionality. Paul Collier, for example, has identified damage to and destruction of physical and human capital, reduction of long term savings, diversion of capital externally (capital flight), economic disruptions and distortion of state expenditures (defense versus social spending) as among the economic effects of armed conflicts. Weapons are deadly and death is irreversible. They are also expensive, often resulting in diversion of precious resources away from social needs. For example, according to SIPRI world and regional military expenditure estimates, from 1991 to 2000 Africa recorded an increase of 20% while the rest of the world (combined) decreased military spending by 11%. Public Expenditures per capita can be even more revealing. In 1990, for example, the ratio of military to health spending was 16:1 in Ethiopia, 10:1 in Chad, 25:1 in Sudan, 4.5:1 in Mozambique and 14.25:1 in Angola. According to the UNDP, the eighty (80) battle tanks Nigeria purchased from Britain in the early eighties came at a cost that could have immunized 2 million children and provided family planning services to 17 million couples. Funny enough since those Tanks arrived, various military regimes in power have been more concerned that they might be used against them internally in a coup rather than as a weapon against Nigeria's alleged external enemies.
One regime even ordered that tracks be removed from the Tanks! Another fact of modern conflict that is often underappreciated is that civilians are much more likely to die than soldiers and children constitute over two-thirds of civilian deaths. Indeed, civilian deaths as a percentage of all deaths in war have reached almost 90% in the nineties, compared with about 15% in the First World War.
WHAT ARE THE DETERMINANTS OF PUBLIC HEALTH?
The factors that determine public health are inter-related. Community health and function are affected by disease as well as the behavioral and biologic responses of individuals in the community.
Community health and function directly impact prosperity and well being both of which in turn affect individual responses. Health care delivery affects individual response, disease and prosperity while disease in turn affects health care. The genetic endowment that individuals are born with, along with the social and physical environment in which they live are influential predictors not just of disease, but also the responses of individuals to disease. But social and physical environment are direct reflections of prosperity. Thus one's best bet is to have good genes and to live in a community of prosperity. But peace is a requirement of prosperity. Investment and development money as we all know is a coward. It does not go where there is trouble. Thus, conflict is antithetical to public health.
As previously noted, bankrupt leadership is a factor in conflict, along with corruption, poverty, lack of peaceful power transfer mechanisms and instability.
In its 2001 report, the African Development Bank analyzed 180 leadership transitions in Africa between 1960 and 1999. Fifty-six (56) percent of leaders left office via coup, war or invasion. Only seven (7) percent left office by losing an election. Just over nine (9) percent left office by natural death, accident or assassination. Another 9% left only because they were tired and chose to retire.
Just under 18% of transitions took place in the context of interim/caretaker governments or impeachment. It seems, therefore, that the predominant focus of African leaders is how to hold on to their jobs with their heads intact. Even without conflict, the African public health scene has certain features, set in Africa's economic milieu, that make the outbreak of conflict even more profound in its consequences. The highest infant mortality rates in the world are in Africa. The lowest disability-adjusted life expectancy (DALE) rates are in Africa. The average number of inhabitants per Doctor is about 15 000:1, ranging from 690:1 in Libya to 57,310:1 in Burkina Faso which is the highest ratio in the world. One observation I have made is that the complex milieu of the African situation makes it difficult to find consistent and direct relationships between conflict, poverty, political stability, economic development and standard indicators of public health. Part of the problem is how we define things. Decalo, for example, defined a stable country as one that, despite some modicum of tension with its armed forces has continued to subordinate them to the political center since independence. Using this definition, today, less than 15 sub Saharan African countries would qualify as 'stable'. These countries and their respective disability adjusted life expectancy (in years) include Botswana (32.3), Malawi (29.4), Mauritius (62.7), Senegal (44.6), Swaziland (38.1), Kenya (39.3), Tanzania (36.0), Cameroon (42.2), Gabon (47.8), Namibia (35.6), Zimbabwe (32.9) and South Africa (39.8). It is obvious from these numbers that factors other than the consistent subordination of the military influence life expectancy. However, the CIA has produced a report on 'The Global Infectious Disease Threat and Its Implications for the United States'. It states that "The relationship between disease and political instability is indirect but real ... infant mortality--a good indicator of the overall quality of life--correlates strongly with political instability"
HEALTH EFFECTS OF WAR
There are many health consequences of war. They include some obvious ones like death, injury and long-term disability. But there is excellent data to show that rape, torture, post-traumatic stress and other long-term mental health problems along with increases in sexually transmitted diseases (including HIV/AIDS) are seen during and after war. Other effects include increases in domestic and sexual violence and crime, increases in communicable diseases (e.g. malaria, meningitis, typhoid, cholera, acute respiratory infections), dislocation of populations, mass migrations (e.g. from rural to urban areas), loss of kin and social networks, influxes of refugees with associated overcrowding, poor sanitation, and environmental degradation. Lastly, deterioration and destruction of health, social, economic and political infrastructures (e.g. reduced or lack of access to basic health prerequisites such as food, shelter, clean water, education, income, health services, social justice) along with widening gaps between rich and poor (e.g. in terms of income, access to health care, health status, living conditions) amplify destructive primary health effects.
ANALYSIS OF IMPACT
Traditionally, we record casualties of war in a system that identifies those were killed in action (KIA), wounded in action (WIA), died of wounds (DOW), non-battle injuries, diseases and accidents, injuries and deaths among prisoners of war, missing in action (MIA). Civilian casualties (also known as collateral damage) usually refer to wounds and deaths directly caused by military equipment. But morbidity and mortality caused by disruption of food and medical systems is often ignored or under reported. An even fuller appreciation of the pervasive and long lasting effects on civil society can be grasped by recognizing that impact can be environmental, physical, chemical, biologic, social, cultural, political, economic, legal and ethical.
HIV/AIDS & CONFLICT IN AFRICA Recent data have highlighted the relationship between the transmission of HIV/AIDS and conflict in Africa.
Violent conflict and HIV/AIDS have both been on the rise in the past decade and the number of states at war or with significant conflicts in sub-Saharan Africa has doubled from 11 in 1989 to 22 in 2000. A recent report claims that "as HIV/AIDS becomes widespread, power struggles over limited resources increase the chance of violent conflict". Warfare is also a well known amplifier of disease. It is said that militias that circulate in war-torn zones sexually harass and exploit displaced populations and contaminate communities and villages when they return to their homes. But the relationship is complex and is certainly not recent. Botswana, which has Africa's highest rates of HIV/AIDS has been at peace and has very high income per capita.
As suggested above, one major area of concern in the relationship of HIV/AIDS to conflict includes the effect on troops and peacekeeping operations. Rates of HIV infection in African militaries may be as high as 60 percent in Angola and the Democratic Republic of Congo and no less but probably even more in Zimbabwe, Namibia and South Africa. The Kenyan Army buries at least two (2) soldiers every week from AIDS. In Nigeria, President Obasanjo announced that 11% of returnee soldiers from West African peace-keeping operations were HIV positive. There is concern in some quarters that even senior officers have not been spared. An unanswered question is whether these returnee soldiers will proceed to contaminate their unsuspecting spouses and girlfriends at home. More recently the UN has made it mandatory for peace keepers to be provided with condoms along with their rifles. HIV screening and counseling are recommended.
However, while most emphasis is on recent patterns of transmission, what I find most intriguing is much more remote. During the Ugandan-Tanzanian border war of 1979, for example, the 207th Tanzanian brigade camped and then advanced from Bugandika to Kyebe to Kyotera to Masaka and on to Kampala. This route of advance later became a well known AIDS trail. It was ascribed to loose sexual activities on the part of the soldiers, but how they got the virus in the first place has never been determined. Unusually high HIV rates among former guerrillas (ANC, ZAPLA, ZANLA, SWAPO etc.) has been a source of concern to me for many years but one has never found a verifiable explanation. Their guerrilla camps were located in east and central Africa (including Tanzania) but they all moved back home when Zimbabwe, Namibia and South Africa became independent. The integrated armies of those countries (along with the never ending war zones of the Great Lakes region) now have the highest rates of HIV/AIDS in Africa. The civilian populations have correspondingly experienced escalating rates of infection.
Other areas of concern in the relationship of HIV/AIDS to conflict include the slowing of economic development and the destabilization of entire societies.
OTHER EFFECTS
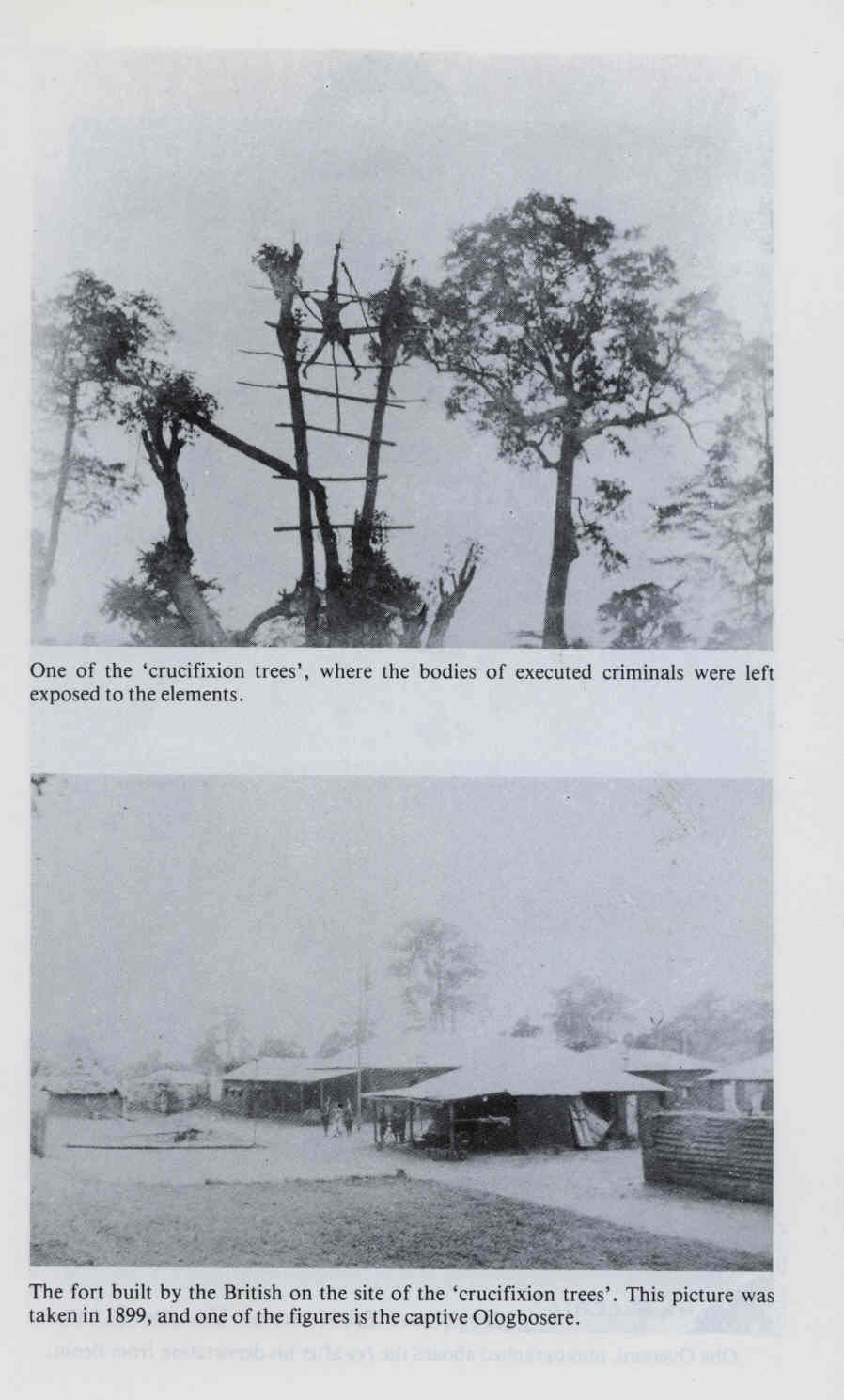
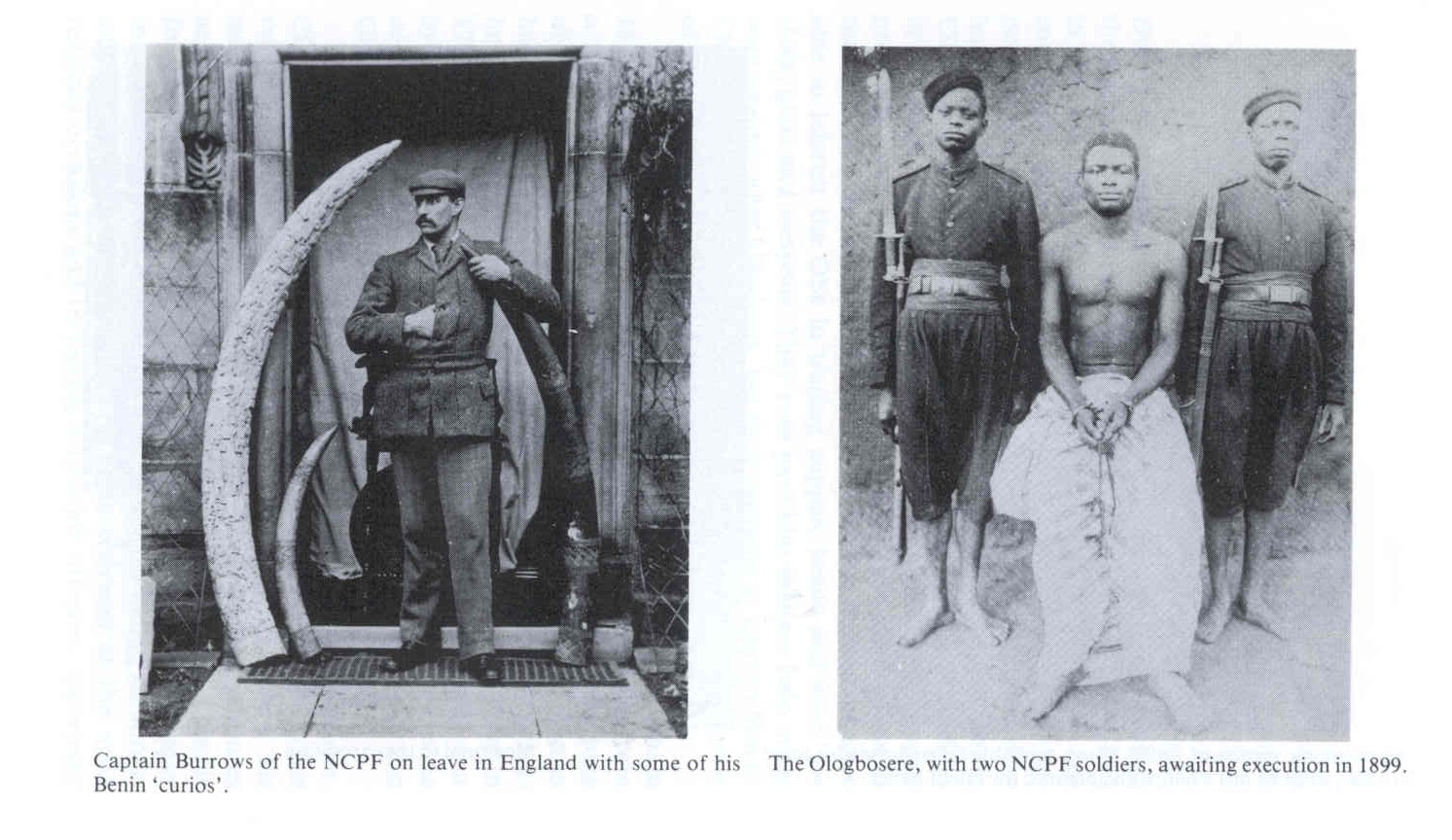
Impact on Human Rights Conflict and war have provided the most serious cases of human rights abuse since slavery. Concentration camps were introduced into warfare during the Boer war. The earliest example of genocide in the 20th century in the world took place in 1904 when the Germans nearly wiped out the Herero of Namibia. In our own Nigeria, some of the actions of Lugard and his henchmen in the early part of the 20th century could qualify as war crimes. During the civil war (1967-70), serious violations of human rights occurred. More recent patterns of civilian casualties at Odi and Zaki-Biam during Nigerian Army internal security operations have certainly raised eyebrows.
But collateral damage from IS operations are not new.
Innocent civilians died during the Maitatsine riots in Kano (1980), Bulumkutu riots in Maiduguri (1982) and Bauchi riots (1990), not to mention subsequent IS operations in Ogoni and Zangon-Kataf. Even during the 'June 12' riots in Lagos, indiscriminate killings took place.
A very good example of the deliberate indiscriminate use of weapons against civilians during war took place during the Italian bombing of Ethiopian civilians in the 1930s. Orgies of ethnic bloodletting occurred in the sixties in Rwanda and Burundi as well as Nigeria (1966). The more recent ethnic cleansing in Rwanda (1994), which resulted in the deaths of 800,000 people in a short time span was on a scale never before imagined in Africa. Indiscriminate use of mines is well established in countries like Mozambique, Angola, and Somalia. Brazen violations of medical neutrality have occurred in Somalia and Sudan where medical clinics, hospitals and first aid stations are routinely attacked by combatants. The use of starvation as a weapon of war was openly canvassed by Lt. Col Mengistu Haile Mariam of Ethiopia in the eighties. Even in Nigeria during the civil war, isolation of the food producing part of Biafra from the rest of the region was the key objective of the final military "link up" that led to its collapse in January 1970. In Sierra Leone, the RUF policy of amputating the arms of young children represents another example of a serious human rights abuse whose ancient origins can be traced to Julius Caesar during his campaign in Gaul.
EFFECTS OF SOME WEAPONS OF MASS DESTRUCTION
The Reganne oasis in Algeria was the site of four (4) atmospheric nuclear weapon detonations between February 13, 1960 and 25 April 1961. In response to outcries from African countries (including Nigeria), testing then moved underground to In Ecker in the mountainous area of Tan Afela at a place called the Oasis Military Test Center. Thirteen underground explosions were conducted until February 16, 1966, before the French testing program was moved to the Mururoa and Fangataufa Atolls in the South Pacific.
The health effects of nuclear weapons usually result from the initial blast, radiant heat and ionizing radiation. Physical injuries, thermal burns and radiation illness are well established effects. But what is less well appreciated are the longer term effects like keloids (disfiguring skin scars), microcephaly (small sized heads) and mental retardation in babies, cataracts, certain types of cancer, and a whole variety of psychological and psychosocial effects.
I am not aware that France ever paid reparations for the atmospheric nuclear tests or that detailed research was ever done to quantify the health effects in Algeria and surrounding nations. Even the effects on underground water tables have never been clarified.
It is intriguing that for a full three and half years after Algeria gained independence, the new governments of Ahmed Ben Bella and Houari Boumedienne actually allowed underground tests to continue. Fortunately, all African nations have since endorsed the 1996 African Nuclear-Weapon-Free Zone Treaty (ANWFZ) of Pelindaba, while most have signed the 1972 Biological and Toxin Weapons Convention (BWC), and the 1997 Chemical Weapons Convention (CWC). In addition, the Bamako Convention on the Ban of the Import into Africa and the Control of Transboundary Movement and Management of Hazardous Wastes within Africa was adopted on 30 January 1991 in Bamako, Mali. While these treaties are not without loopholes, the direction (from a public health standpoint) is positive. Notable examples of the use of weapons of mass destruction in African conflicts include Rhodesian counter-insurgency airdrops of Anthrax spores against ZANLA and ZAPLA guerillas from 1978-80 causing 10,000 civilian illnesses and 182 deaths as well as negative effects on rural food production. More recently, Libya was accused of deploying chemical agents against Chadian troops in 1987. Even now Libya is still suspected of having a chemical weapons capability.
The (false) presumption that one has weapons of mass destruction can also lead to undesirable consequences for public health. On August 20, 1998, for example, as part of "Operation Infinite Reach", in response to the US Embassy bombings in East Africa, the U.S. fired Tomahawk cruise missiles at the al-Shifa Pharmaceutical Factory in Khartoum, Sudan. The destruction of the plant seriously affected the local production of medicines for the Sudan national health system. But it turned out to be based on faulty intelligence from a soil sample that allegedly revealed the presence of EMPTA, a precursor of a nerve agent called VX.
Most people do not realize that "common" tear gas used by the Police forces of many African nations (including Nigeria) as a harassing agent is a form of chemical warfare and that it can lead to serious respiratory illness and death. No less than 80 countries have requested that tear gas be added to chemical weapons banned by the Geneva protocol. Most tantalizing of all is the scenario of "race based weapons". In apartheid South Africa, for example, research into race specific bio-weapons was actively conducted under the direction of Dr. Wouter Basson at the Roodeplaat Research Laboratories. It has been officially acknowledged by researchers in Europe that modern genetic techniques can lead to the development of designer weapons that target certain genetic differences between ethnic groups. We certainly cannot afford such misuse of technology in Africa.
PRODUCTION, STORAGE, TESTING AND DISPOSAL ISSUES
Weapons acquired for conflict can cause public health effects in peace time merely as a result of production, storage, testing and disposal. The recent ammo dump explosion at Ikeja cantonment in Lagos, Nigeria comes to mind. Most of the over 1000 casualties were children.
In Kenya, Kikuyu nomads have complained for many years about deaths and injuries from unexploded munitions left over after military exercises conducted by the British Army. SMALL ARMS According to Oscar Arias Sánchez, "All studies indicate that, in both the military and criminal sphere, the greatest percentage of violent deaths occur from the use of light weapons and small arms." The widespread availability of small arms and weapons helps to fuel conflicts and tilt nonviolent disputes into violence. There are numerous initiatives in progress to stem this problem. In Africa, relevant efforts include the UN Conference on the Illicit Trade in Small Arms and Light Weapons, United Nations Institute for Disarmament Research (UNIDIR), The Wassenaar Arrangement, United Nations General Assembly Resolutions and Reports and the Organization of African Unity.
The UN Conference was held from 9-20 July 2001 in New York and was attended by delegations from many African countries including Nigeria. A Program of Action was agreed upon but it turned out to be very watered down as a result of concerns expressed by the US delegation. A review conference is planned for 2006.
MINES Although cheap to produce, mines are one of the most deadly and long-lasting forms of war with serious public health effects. When deployed on or near farmland and streams, farming activities are paralyzed, resulting in food shortage and malnutritionrelated diseases. The contamination of drinking water causes waterborne diarrheal diseases.
Denial of road use and access to communities affects rural public health campaigns like vaccination drives.
Physical injuries lead to amputation and blood transfusion. In an environment with contaminated blood, this increases the risk of diseases like malaria, hepatitis and AIDS. Six countries in Africa remain outside the Mine Ban Treaty. They are Central African Republic, Comoros, Democratic Republic of Congo, Eritrea, Nigeria, and Somalia.
Twenty-six countries, in addition to Somaliland, are mine-affected. These countries include Angola, Burundi, Chad, Congo-Brazzaville, Djibouti, DR Congo, Eritrea, Ethiopia, Guinea-Bissau, Kenya, Liberia, Malawi, Mauritania, Mozambique, Namibia, Niger, Rwanda, Senegal, Sierra Leone, Somalia, Sudan, Swaziland, Tanzania, Uganda, Zambia, and Zimbabwe.
REFUGEES
According to the UNHCR, of the 21,793,300 refugees in the world, 6,072,900 are in Africa alone, constituting the second largest group. Asia has 8,450,000 displaced persons; Europe 5,571,700; North America 1,047,100; Latin American & Caribbean 575,600 and Oceania 76,000.
SEXUAL VIOLENCE
For obvious reasons, limited official statistics exist on this problem. But the recent disclosure of an Aid-for-Sex scandal among some NGOs in Africa has highlighted the issue. Most women and children are too scared to bring charges against their assailants for fear of reprisals. Fighting militia, Peace Keepers and humanitarian workers have all been implicated. In Sierra Leone for example, a 1999 study found 1862 female victims of sexual abuse during the January 1999 offensive against Freetown. 55 percent of them were gang raped and 200 got pregnant.
A related issue is the question of fatherless children of war. Nigerian peace-keepers serving with ECOMOG, for example, were alleged to have left 22,000 babies behind when they departed Liberia.
FOOD SUPPLY AND CROP PROSPECTS
According to the FAO, as of December 2000, some 28 million people in sub-Saharan Africa were facing severe food shortages. Eastern Africa (Eritrea, Ethiopia, Kenya and Sudan) was the most precarious due to the combined effects of drought and/or civil strife
CHILD SOLDIERS IN AFRICA
Armed conflict affects children in many ways. They include effects on health and nutrition, psychological recovery and social reintegration, education, recruitment as child soldiers, consignment to refugee camps, gender-based violence, landmines and unexploded ordnance and neglected adolescence. It is estimated that about 300,000 children are currently participating in fighting, in more than 35 countries. The recent ratified UN Convention on the Rights of the Child bans children less than age 18 from being drafted into combat. It came into force on Tuesday Feb 12, 2002.
Conflicts in the many African countries have utilized the services of child soldiers either on the government or rebel side. They include Algeria, Angola, Burundi, Chad, Republic of Congo, DRC, Eritrea, Ethiopia, Rwanda, Sierra Leone, Somalia, Sudan and Uganda
UNICEF'S ANTI-WAR AGENDA
In 1996, as part its annual report on the State of the World's children, UNICEF outlined a ten point agenda against war. The areas of focus include prevention, girls and women, child soldiers, land mines, war crimes, children as zones of peace, sanctions, emergency relief, rehabilitation and education for peace.
HUMANITARIAN ASSISTANCE AND CONFLICT
The issue of humanitarian assistance during African conflicts is not as straightforward as meets the eye.
Points of controversy include control of supplies intended for civilians, the opportunity-benefit for War Lords of local resource diversion for war making, ethics, political neutrality, and conditionality for granting access to held territories. Other issues include professionalism and training among some AID workers and organizations, peace building, post-conflict rehabilitation of Health Services, health services auditing and management, human resource identification and management, infrastructure and financing. The process of peace-building requires a definition of roles and responsibilities of actors, as well as addressing issues of equity, access, effectiveness, efficiency, appropriateness and sustainability.
PUBLIC HEALTH POLICY ISSUES
The broad field of public health policy in conflict and war is relatively new. Many issues need to be addressed through formal research, consultation and collaboration. Limitations of current approaches include a focus on reactive interventions rather than on proactive interventions, a focus on short-term relief and rehabilitation activities (e.g. the provision of food, water and emergency medical services) rather than on longer-term development activities; a focus by international agencies and governments on the provision of medical equipment and supplies and restoration of the health infrastructure to its pre-conflict state, with little emphasis placed on redefining the organization and structure of the health system; a dearth of agencies carrying out both relief and development activities; as well as lack of coordination and collaboration among donors and non-governmental organizations in relation to peace building and reconstruction activities. There is need to put in place "early warning mechanisms" at the international level to monitor the disintegration of legal, political and social structures that increase the likelihood of violent conflict so that we may intervene before large-scale violence erupts.
Other issues include the paucity of input of internal (e.g. indigenous) actors in conflict resolution and peace building activities; only recent acknowledgement by some groups of the importance of conflict resolution activities as part of the peace building and health development process; the rarity of formal evaluations of work in post-conflict situations including research and assessment of health interventions undertaken by NGOs in relation to peace building, meeting of needs and contributing to the development of larger health policy frameworks.
UN RECOMMENDATIONS
In his landmark presentation titled "The causes of conflict and the promotion of durable peace and sustainable development in Africa", UN Secretary-General Kofi Annan made recommendations addressing many components of the problems of conflict in Africa. These recommendations directly impact Public Health and should be viewed as a grand strategic template from which operational details can be derived. As outlined by APIC, Annan proposed:
'ON ARMS AND ARMS TRAFFICKING
1. United Nations Member States should pass laws enabling prosecution in national courts of violations of Security Council arms embargoes.
2. The Security Council should urgently consider how the United Nations might help compile, track and publicize information on arms trafficking.
3. African governments should reduce purchases of arms and munitions to 1.5 per cent of gross domestic product (GDP), and maintain zero-growth on defence budgets for the next decade.
ON SANCTIONS:
1. Economic sanctions are too often a blunt instrument, and should be better targeted, for example, by freezing the assets of decision makers, their organizations and their families and through restrictions on travel.
2. Combatants should be held financially liable to their victims under international law where civilians have been deliberately targeted 3. International legal machinery should be developed to help find and seize the assets of the transgressors
ON REFUGEES:
1. An international mechanism should be established to help host governments maintain the security and neutrality of refugee camps. Such camps should be located away from borders; combatants should be separated from genuine refugees.
ON STRUCTURAL ADJUSTMENT:
2. The Bretton Woods institutions should consider providing "peace-friendly" structural adjustment programs.
3. Conditionalities must not be antithetical to a peace process; donors should not cut off funds from a weak government making good-faith, popularly supported efforts to implement peace agreements.
ON DEVELOPMENT ASSISTANCE:
1. Aid should be restructured to focus on high-impact areas (rural water supply, basic education, primary health) and to reduce dependency.
2. Donors should strive to ensure that at least 50 per cent of their aid to Africa is spent in Africa.
3. New sources of funding are required from donor countries.
ON DEBT AND TRADE:
1. The scope of the Highly Indebted Poor Countries initiative of the World Bank and International Monetary Fund should be greatly expanded, since only four African countries have so far met its conditions.
2. All creditors should convert into grants all remaining official bilateral debt of the poorest African countries.
3. Creditors should consider clearing the entire debt stock of the poorest African countries, as requested by the OAU.
4. The next summit of the Group of 8 industrialized countries should consider eliminating trade barriers to African products.
ON THE SECURITY COUNCIL
1. The Security Council should meet every two years at ministerial level to assess efforts undertaken and actions needed to support peace and development in Africa.
2. The Council should consider convening, within five years, a summit-level session for the same purpose.
ON INTERNATIONAL BUSINESS PRACTICES:
1. Countries implementing the Convention Combating Bribery of Foreign Public Officials in International Business Transactions should set a timetable for early enactment of national legislation.
2. The OAU should draw up by the year 2000 an African convention on the conduct of public officials and the transparency of public administration.'
CONCLUSION
Conflict in Society is a Public Health Issue. Public Health trainees, organizations and professionals should acquire skills for conflict mediation and prevention of war. Through education, advocacy and direct participation they can help deal with what is obviously the most serious threat to public health.
If war has begun, professionals and organizations should work to limit the health and environmental consequences. When war ends, professionals and organizations should care for victims and strive to minimize the long term health consequences of war.
_____________
REFERENCES
African Development Bank: African Development Report 2001. Oxford University Press 2001.
Pamela Thompson, INPRO Consulting Inc. (August 2000) Position Paper: Peace and Health.
http://www.csih.org/papers/peacehealth.html Africa: Secretary-General's Report to the UN Security Council
http://www.un.org/ecosocdev/geninfo/afrec/sgreport/ (April 1998) Levy and Sidel (eds): War and Public Health. Oxford University Press 1997 Africa Policy Information Center
http://www.africapolicy.org/index.shtml UN Security Council, breaking tradition, takes up AIDS http/www.oneworld.org/ips2/jan00/17_49_075.html Smock DR. Humanitarian Assistance and Conflict in Africa
http://www.jha.ac/articles/a014.htm Graça Machel: Impact of Armed Conflict on Children
http://www.un.org/rights/introduc.htm Humblet, P. & Biot, M. (undated) MSF Programmes in Post-conflict situations. Paper prepared for 'Post-conflict health policy and planning workshop', organized by the Health Policy Unit, London School of Hygiene and Tropical Medicine, 4-5 February 1999.
Unpublished manuscript.
Humblet, P. & Biot, M. (1999) MSF Programmes in Post-Conflict Situations. Belgium: Médecins Sans Frontières.
London School of Hygiene and Tropical Medicine (October 1999) From conflict to peace - transitions in health policy and planning , A Report of the World Bank. London:LHSTM.
World Bank (1998) Post-Conflict Reconstruction: The Role of the World Bank. Washington: World Bank USIP Report: HIV/AIDS and Conflict in Africa http://www.usip.org/pubs/specialreports/sr75.html.
Landmines Monitor Report, Full Report http://www.hrw.org/reports/1999/landmine/
RETURN


© 2025 Segun Toyin Dawodu | All rights reserved
